Arthritis is a common joint disease involving pain, stiffness, swelling and inflammation resulting from a breakdown of the cartilage lining in the joint. Osteoarthritis (OA), the most common type of arthritis, is regarded as a “wear and tear” condition and can only progress with currently no existing cure to replace the cartilage lining. Additionally, there are over 100 types of arthritis caused by systemic conditions such as gout, rheumatoid arthritis, psoriatic arthritis, lupus, etc.
Knee osteoarthritis is the most common form of OA, affecting over 26.9 million Americans yearly. It is estimated that 15% of individuals over 45 years old suffer from knee OA, with that number increasing to 33.6% for those older than 65 years. It is also a major global burden to public health, resulting in an estimated cost of $27 billion dollars annually. Knee arthritis can be extremely debilitating and cause severe pain, swelling, deformity, instability, and adjacent muscle weakness. It can severely impact our ability to walk and perform daily activities and exercises.


Fig.1 – Left, comparison Xray of knee with no arthritis; Right, Xray of knee with advanced arthritis, worse in the medial compartment
The etiology of osteoarthritis is complex and multifactorial, and includes such factors as age, weight, familial history, job type, previous trauma, sports and exercise regimens. Eventually, the cartilage may deteriorate down to the bones which then start rubbing on each other (“bone-on-bone”) (fig.1). This is known as severe or end-stage osteoarthritis. When this happens in the knee, large bone spurs can develop and the alignment of the knee and leg may change from straight to bowed in or outward (fig.2). On imaging, knee arthritis is diagnosed with x-rays; a MRI may sometimes be helpful to characterize the extent of arthritic change if not already evident.


Fig 2. Left, Valgus knee (knock-knee); Right, Varus knee (Bow-legged)
Conservative treatment options revolve around rest, activity modification, weight loss, anti-inflammatory medication, physical therapy and injections. Given its progressive nature, the arthritic knee may stop responding to these treatments over time. Also, knee arthritis may be further complicated by degenerative meniscus tears, which can be seen in up to 90% of people with arthritis and can exacerbate arthritic symptoms.
What happens when these conservative treatment options no longer provide relief? In these cases, surgical options are usually discussed. The indications for each procedure vary, but the common thread is that surgery is recommended when nothing else works. However, surgery can instill anxiety in patients because of the unknowns surrounding these procedures and the recovery associated with it. The purpose of this article is to briefly explain some of the surgical options used to treat knee arthritis.
Arthroscopy with Bone Void Filler
As the cartilage wears down and arthritis progresses, the underlying bone can be affected. This may result in changes such as bone marrow edema (“bone bruise”) or even an underlying subchondral fracture (“stress” or “insufficiency” fracture). When these changes occur an arthroscopy may be indicated, supplemented with a bone void filler. This involves injecting a calcium or bone-like substance within the bone to fill the damaged bone area (fig.3). This substance is usually incorporated into the surrounding bone with no allergy or rejection. As with routine arthroscopy this procedure is not definitive and will not alter the cartilage or bone, so symptoms may return in the future.
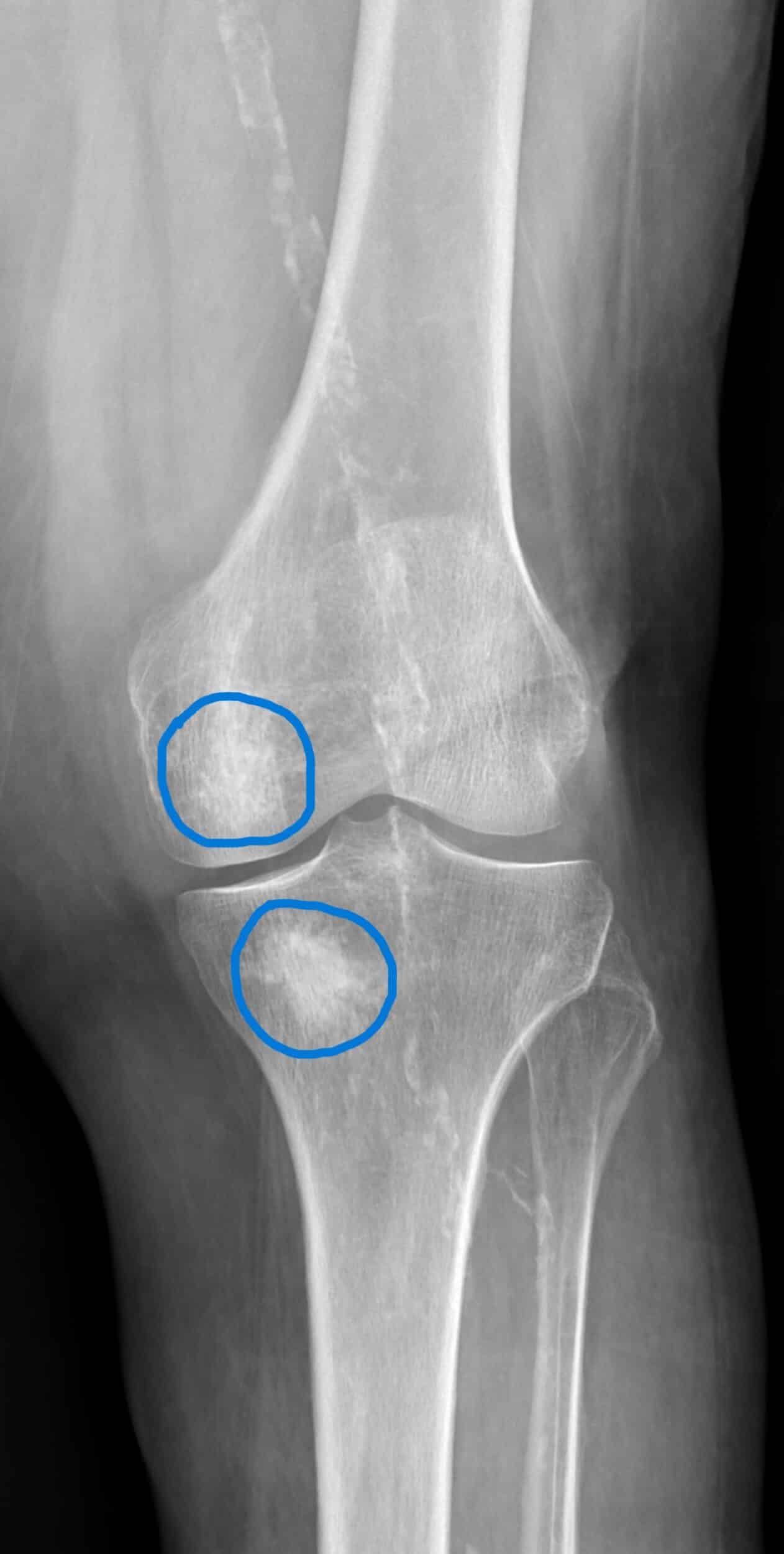
Fig 3. Knee after bone void filler placement (circled)
Osteotomy
As mentioned earlier, arthritis progresses and the bony alignment changes causing worsening pain, deformity, and instability. An osteotomy is a surgical procedure to cut and realign the bone to a more anatomic state. This is usually done at the proximal tibia or distal femur (fig.4). Osteotomies are useful not only in correcting deformities but also in offloading the affected knee compartment. These procedures can be done in conjunction with others such as cartilage restoration, ligament reconstruction, meniscus repair or transplant. However, while osteotomies are an effective treatment option, they are contingent upon good bone quality and healing. They may also not be effective in severe end-stage osteoarthritis if the deformity is too great. Thus, osteotomies are typically reserved for younger patients who have suffered early onset arthritis or may not yet be candidates for knee replacement.

Fig 4. Knee after medial opening wedge high tibial osteotomy
Partial knee arthroplasty
Arthroplasty, or knee replacement, is typically reserved for end-stage osteoarthritis when a bone-on-bone appearance is noted. There are 3 main compartments within the knee and occasionally the worst arthritic changes may be limited to one compartment. In cases of isolated unicompartmental disease the patient may be a candidate for a partial knee replacement, which replaces the arthritic bone and cartilage with metal and plastic prostheses (fig.5). When indicated partial knee replacements may be a more attractive option to total knee replacement, as it maintains most of the native knee and the kinematics of the knee are better preserved (i.e. may feel like a more “normal” knee). Additionally, recovery time is usually shorter than a total knee replacement. However not every patient is a candidate for partial knee replacement, as arthritis typically affects the entire joint.

Fig 5. Knee with medial partial knee replacement
Total knee arthroplasty (TKA)
A total knee replacement is performed when a patient has end-stage arthritis in all compartments of the knee and has failed conservative treatment. To simplify, the ends of the diseased portions of bone and cartilage are carefully removed and resurfaced with a metal prosthesis. A plastic spacer is inserted between the bones, allowing movement at the joint (fig.6). Along with arthroscopy, joint replacement is one of the most common orthopaedic knee procedures performed globally. It has been proven as an effective, reliable, and durable treatment option for end stage arthritis. Satisfaction rate is high, with literature showing ~85-90% satisfaction rate and 90-98% survivorship at 10 yrs. These numbers decrease with younger patients, possibly due to increased activity level and expectations. Over the years, advances in technology have led to robotic-assisted and navigated TKA. With these modalities surgeons can now construct a pre-operative plan using software and perform the surgery with computer guidance, possibly resulting in more accurate and reproducible bone cuts. Improvements in anesthesia protocols and pain management have also resulted in TKA being done as a same-day or overnight procedure.

Fig 6. Knee with total knee replacement